A fracture is a break in the bone that is caused by an external force. Depending on your age and the strength of your bone, the amount of force required to cause a fracture may vary considerably.
Geriatric fractures, also known as fragility fractures or osteoporotic fractures, are typically low-energy injuries that occur in older patients who have lower bone density or hormonal deficiencies. Geriatric fractures can occur after minor falls or seemingly trivial injuries during normal daily activities, which would not ordinarily cause fractures in a younger person. These geriatric or osteoporotic fractures most commonly occur at the hip, wrist (distal radius), backbone (vertebrae) and shoulder (proximal humerus).

The bones in our body are in a constant state of flux — new bone is produced in response to stress and old bone is broken down due to disuse. In young people, new bone is made at a faster rate than old bone breaks down, resulting in a high bone mass. After the early 20s this diminishes, hence peak bone mass is usually reached by the late 20s, after which, bone begins to be lost faster than it can be produced. Eventually, this can lead to osteoporosis in later life.
How likely you are to develop osteoporosis depends partly on how the peak bone mass you attained in your youth. The higher your peak bone mass, the more bone you have “in the bank” and the less likely you are to develop osteoporosis as you age. Peak bone mass is affected by gender, race, genetic inheritance, nutritional status and hormonal factors. People who reached lower levels of peak bone mass in their younger years have a higher chance of developing osteoporosis as they age, putting them at greater risk of osteoporosis and geriatric fractures.
Geriatric fractures can greatly affect one’s quality of life, often resulting in chronic pain and a loss of independence and mobility. Some patients may even require round the clock care or have to move into an assisted living facility if mobility is severely affected, for example, after a hip or vertebral fracture.
Age is the biggest risk factor for geriatric fractures. Startlingly, an 85-year-old is at four times higher risk of getting a geriatric fracture than a 75-year-old! There is a laundry list of risk factors for geriatric fractures, which can be divided into modifiable and non-modifiable risk factors.

Modifiable risk factors are factors that you can change and control, to alter the likelihood of getting a geriatric fracture. These include:
Non-modifiable risk factors are factors that contribute to your risk of getting geriatric fractures, but unfortunately cannot be changed:
When you hear the word fracture, you would normally associate it with severe pain and the inability to move the fractured bone. However, geriatric fractures do not always cause severe pain or disability, which makes the condition more insidious and harder to detect and treat.
Common symptoms:
During your consultation, your doctor will ask you about the events surrounding the geriatric fracture, assess for the presence of the aforementioned risk factors, and conduct a physical examination to ascertain the site and severity of the geriatric fracture.
To confirm the diagnosis, additional scans are required. These include X-rays, CT and/or MRI scans of the affected area, as well as any other parts of the skeleton your doctor suspects may have concomitant fragility fractures. A special DEXA (Dual-energy X-ray absorptiometry) scan will be performed to assess the density of your bones, which directly correlates to the risk of osteoporotic geriatric fractures.
In some cases, if your doctor suspects an underlying condition causing increased bone fragility, various blood tests to assess mineral and vitamin levels (calcium, phosphate, Vitamin D) and other organ functions (thyroid, kidney function tests) may be done as well.
In general, treatment for geriatric fractures can be divided into conservative and surgical options, depending on the location and severity of the fracture, and how badly it affects the patient’s function and quality of life.
Conservative treatment includes painkillers, supplements (calcium, Vitamin D), physical rehabilitation as tolerated, and medications (to increase bone density) to prevent worsening of osteoporosis. Regular weight-bearing exercise and a nutritionally balanced diet are important in improving bone density and treating osteoporosis.
Below is a brief overview of how some of the more common geriatric fractures are managed, and what you can expect during these treatments.

Hip fractures are one of the most common, disabling and painful geriatric fractures, and often have to be treated by surgery to restore function and alleviate the pain. Non-surgical management is normally reserved for patients who were already unable to walk before the injury and who have medical problems placing them at high risk during surgery. Hence, the vast majority of hip fractures require surgery to allow the patient to return to independent ambulation and daily activity.
The type of surgery depends on the location and severity of the hip fracture, as well as the patient’s age and desired level of activity after the operation.
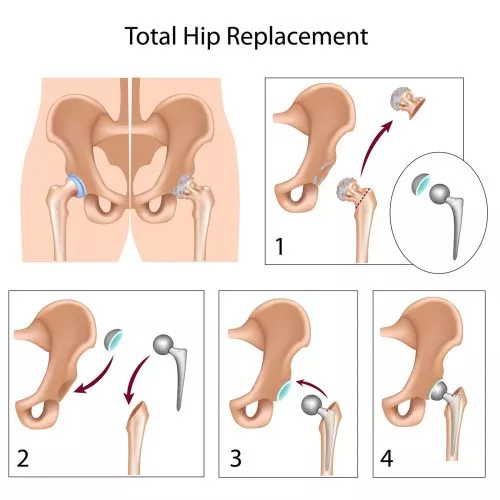
In some patients with less severe fractures, surgical fixation with screws (e.g. cancellous screws, dynamic hip screws) will be sufficient to stabilise the fracture. For more severe fractures that are unlikely to heal even with surgical fixation, either a partial or total hip replacement are typically recommended to replace the fractured bone and restore joint stability and mobility. Patients who desire a more active lifestyle usually benefit from a total hip replacement to restore maximum hip function; on the other hand, older and more sedentary patients can opt for a partial hip replacement (hemiarthroplasty), which is a quicker and simpler operation that can be performed by most orthopaedic surgeons.
Total hip replacement surgery is somewhat more complex than partial hip replacement and is best performed by a subspecialised hip surgeon, who can offer the most current and advanced surgical techniques to minimise complications and maximise recovery.
In patients with multiple health conditions, limited mobility or a short remaining life expectancy, surgery may not be recommended, and painkillers will be the mainstay of treatment.
Wrist fractures, particularly distal radius or Colles’ fractures, are usually sustained when falling on an outstretched hand.


Shoulder fractures involve a fracture in the upper arm (humerus) near the shoulder, usually caused by falling on an outstretched hand.


If the fracture has multiple fragments or is severely displaced, surgery is often indicated. The type of surgery may vary, but in general, metal plates and screws will be inserted to hold the bone fragments stably in place. This will allow optimal healing and prevent deformities or disability in the fractured arm in the long run. For very severe fractures, a partial or total shoulder replacement is sometimes the best option to reliably restore shoulder movement and function.
Geriatric fractures are often associated with numerous complications, as the bone fragility these patients makes surgery more challenging, and the relatively advanced age of these patients sometimes resulting in a more prolonged or complicated recovery process.


If you or your loved ones have symptoms similar to what has been described above, they may be at risk of or already have geriatric fractures. Prevention of geriatric fragility fractures is always better than cure, and it is important to see your doctor early for screening of osteoporosis, which typically comprises of a simple blood test and bone mineral density (BMD) scan. If osteoporosis is detected, there is medication available for effective treatment of this condition, which can significantly lower the risk of osteoporotic geriatric fractures. Herein lies the importance in seeking an early consult.
If the unfortunate happens and someone you know sustains an osteoporotic geriatric fracture, please seek help from your orthopaedic surgeon as soon as possible and get advice on the most suitable treatment option. Early diagnosis and treatment often lead to the best results, with early recovery and more rapid return to function and daily activities!
Our friendly team is here to serve you. For urgent enquiries and appointment requests, please call or WhatsApp us directly.