
If your knees are painful and stiff, and regular pain medication isn’t helping anymore, you may have knee arthritis and you should consult with your doctor if knee replacement surgery is needed.
We’ll be giving you a quick overview of the Oxford Partial Knee Replacement using Minimally Invasive Surgical (MIS) techniques, as well as its benefits, risks and how it differs from a Total Knee Replacement (TKR). This will help you to make a more informed decision about which surgery will benefit you the most.
[Note: Partial knee replacement surgery is often interchangeably referred to as Unicompartmental Knee Arthroplasty (UKA)]

Knee replacement surgery is typically performed for people with arthritis of the knee joints. In older patients, arthritis is commonly caused by degenerative wear and tear over decades of use. Younger patients, on the other hand, typically develop arthritis after poorly-healed injuries (cartilage injury) from sports or trauma.
The pain, stiffness and functional impairment caused by arthritis can be debilitating and extremely frustrating for patients, especially those who lead active lifestyles, travel regularly, or enjoy going out to meet their friends and family.
If you have already tried treatments such as heat or cold packs, knee injections (such as joint lubricants and steroids) or painkillers, but the pain is still significant, then the next step could be knee replacement surgery.
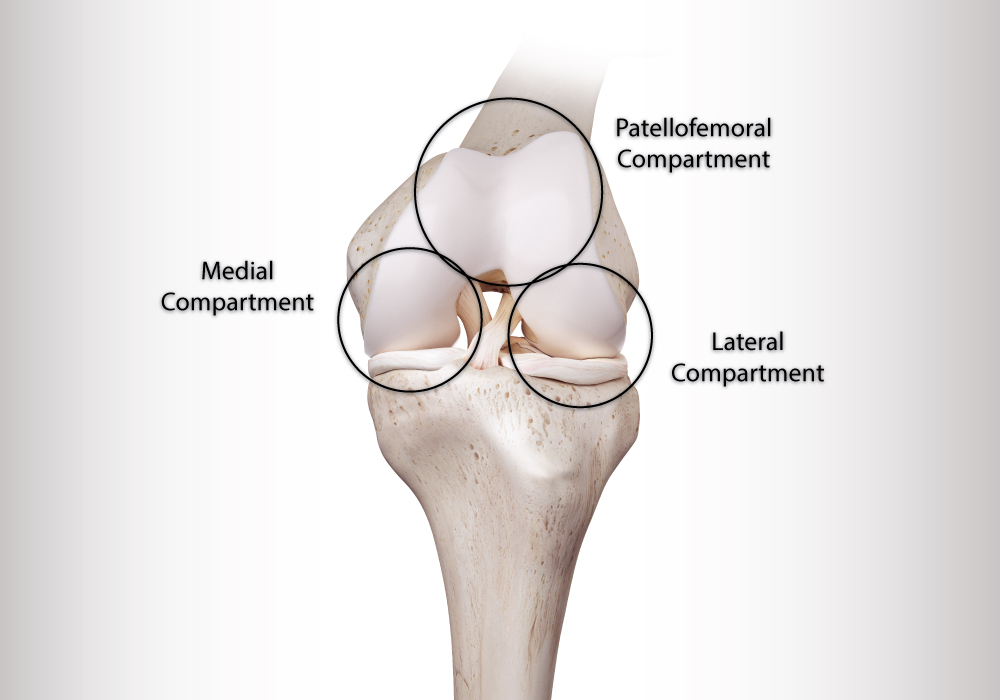
The knee joint comprises three compartments – the medial (inner), lateral (outer) and patellofemoral (front) compartments. Arthritis can occur in any one of these compartments, and sometimes affects two or even all three compartments. However, approximately 80-90% of patients first develop isolated medial-sided (inner-sided) knee pain, and these patients are often suitable for partial knee replacement (UKA).
To accurately assess which compartment is affected, your doctor will perform a knee X-ray, and this will help diagnose which area of the knee joint is most affected.
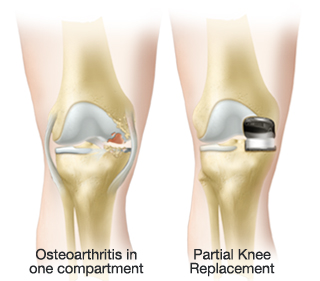
The Oxford Partial Knee Replacement system utilises a relatively small implant to replace the medial compartment of your knee joint and is recommended for patients with knee arthritis that is confined to the medial compartment (inner side) of the knee joint.
Unfortunately, this means that not all patients with knee arthritis will be able to undergo a partial knee replacement (UKA), since late-stage arthritis can affect multiple compartments, which would require a total knee replacement surgery (TKR) instead. However, up to 40-50% of patients with knee arthritis are suitable for Oxford Partial Knee Replacement. Hence it is important to see your doctor early when experiencing knee pain!
The Oxford Partial Knee Replacement system is a sophisticated knee implant that is significantly smaller than implants used in a TKR, and comes with various enhancements that will restore your knee’s function and maintain a natural feeling when using the knee. It has been shown to better restore knee range of movement and provide a more natural-feeling knee when compared to TKR.
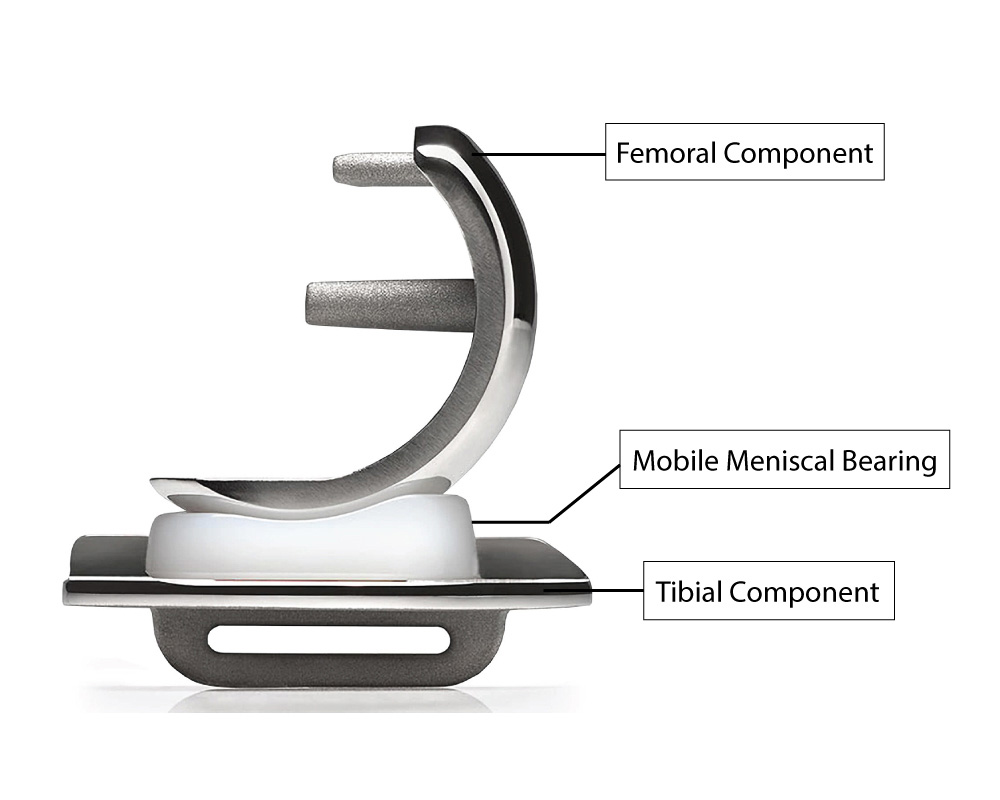
The Oxford Partial Knee Replacement implant comprises 3 components – femoral and tibial metal components, and a polyethylene mobile meniscal bearing. Its special features include:
- Stability – The top and bottom components of the implant, which will be attached to the femur and tibia (the top and bottom parts of your knee joint), are specially designed to fit precisely into the bone, providing greater stability and durability.
- Durability – The smooth highly polished surface of the implant reduces the amount of friction and stress, making the implant more durable. The Oxford Partial Knee uses a special coating that promotes ingrowth of bone into the implant, and does not require the use of bone cement for fixation (unlike most other partial knee replacement systems). This improves the longevity of the Oxford implant when compared to conventional cemented partial knee implants.
- Smooth joint movement – The unique mobile meniscal bearing replicates the function of knee cartilage, allowing for more fluid and seamless motion of the knee joint. This mobile bearing in the Oxford Partial Knee experiences less stress than fixed bearings in conventional partial knee implants and undergoes less wear over time.
The surgery is carried out using Minimally Invasive Surgical (MIS) techniques. Compared to a conventional total knee replacement (TKR), partial knee replacement utilises a skin incision that is approximately half the length, with significantly less damage to the muscle, ligaments and soft tissue around the knee. Additionally, the undamaged lateral and patellofemoral compartments of the knee are preserved, together with all the major knee ligaments, and this provides a more natural-feeling and mobile knee compared to total knee replacement.

Before the surgery, you will be thoroughly examined by your surgeon to confirm that you are suitable for partial knee replacement. X-rays will be done for your surgeon to plan the ideal site and positioning of the knee implant according to your unique knee anatomy.
During the operation, a short incision will be made along the inner side of your knee, followed by removal of the damaged bone and cartilage to create space for the Oxford Partial Knee Replacement implant to be fitted into place. After checking that the implant’s location is optimal and allows for the best range of motion of your knee, the wound is closed and the operation is completed. Most patients recover quickly and many are able to walk on the same day after surgery!
After the operation, you will typically have to undergo physiotherapy for rehabilitation for around 4-6 weeks, after which you will likely be able to resume normal activities. This is almost half the usual recovery time for a total knee replacement (TKR), and is achieved using MIS partial knee replacement (UKA) techniques.
As with most knee implants, approximately 90% of Oxford Partial Knee Replacement implants are still functioning well after 15 years, depending on the patient’s level of activity and usage of the replaced joint. This is comparable to TKR implants.
Choosing the Oxford partial knee replacement confers multiple benefits:
- Shorter hospital stay
- Faster recovery time
- Excellent long-term results
- More natural feeling knee with better range of movement
- Lower risk of post-operative complications
- High patient satisfaction
As with any operation, there are still some potential risks, although these are rare. These risks apply to both total and partial knee replacement surgeries:
- Infection
- Loosening of the implant
- Fracture of the bone around the implant
- Wear and tear
- Dislocation
- Injury to surrounding neurovascular structures (very rare)

An Oxford Partial Knee Replacement removes up to 75% less bone and cartilage compared to a total knee replacement (TKR), resulting in less post-operative pain and swelling. The implant inserted is considerably smaller as well, meaning that there is less damage to your bone and soft tissue during the operation, allowing for faster recovery. Large studies have also shown that partial knee replacement (UKA) is safer, with lower complication rates than TKR.
In a TKR, two knee ligaments (ACL & PCL) that are important for maintaining knee stability are often removed, but in an Oxford Partial Knee Replacement, they are preserved intact, so your knee will have greater stability, better range of motion and retain a more natural sensation (proprioception).
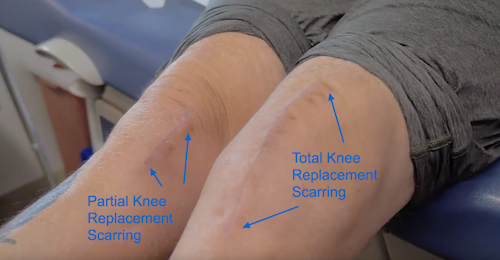
Additionally, the scar from a partial knee replacement (UKA) is more cosmetically pleasing, as it is shorter and on the inner side of the knee, as opposed to a TKR scar, which is a large vertical scar over the front of the knee.
Various clinical studies also reported higher patient satisfaction with their ability to perform daily activities, as well as a quicker return to low-impact sports, when compared against patients who underwent TKR.
If you have painful arthritis that affects mainly one side of the knee, you may be suitable for a partial knee replacement (UKA). You should discuss the pros and cons of both total and partial knee replacement surgery with your doctor, who will guide you in making the best decision for your knee.